




































General information
Diseases of the human musculoskeletal system, such as osteochondrosis, essentially degeneration of articular cartilage and nearby bone tissue, often involving adjacent blood vessels, muscles, and nerve endings. BAN BENE In principle, this term can refer to a number of osteoarticular pathologies of various localities, including the joints of the limbs, but is most commonly used to denote degenerative-dystrophic changes in structure. directly on the spine and especially on the intervertebral discs.
As intervertebral osteochondrosis progresses, the human body loses its shock-absorbing properties, inherent mobility, and flexibility. In general, this spinal disease is very common and a degree of severity is already present in most people by the age of 40. In clinical practice, a distinction is made between cervical, lumbar, and thoracic osteochondrosis, depending on the segment of the spine involved, as well as their mixed forms, which are considered the most severe.
Osteochondrosis of the thoracic spine, which will be discussed in this article, is the rarest form of pathology, due in particular to the anatomical structure of the upper part of the human skeleton. Thus, in the thoracic region, the bone-cartilage system consists of 12 vertebrae connected by joints with ribs that connect their anterior end to a relatively monolithic sternum. Such a skeletal structure is a sufficiently rigid and strong frame that protects the organs of the thoracic cavity (heart, lungs) from injury. In addition, the vertebrae of this segment of the spinal column are characterized by the low height and significant length of the vertebrate processes, which allows viewing of tightly spaced tiles. Together, this limits the mobility of this part of the back and the negative effects of physical activity on it, protecting the intervertebral discs from destruction.
Another reason for the lower incidence of osteochondrosis in the chest compared to lumbar and cervical osteochondrosis is physiological kyphosis (natural backward bending of the spine) in this area, which causes most of the external load on the anterior and posterior vertebrae. falls on the side fragments. With the development of the pathological process in the spinal movement segment, these areas are primarily degenerative, but due to the lack of nerve endings and spinal membranes, pain is most often not observed. Nevertheless, in some cases, negative transformations in the thoracic segment of the spine are affected by plates and posterior fragments of the vertebrae and / or the vertebral-rib joints, often leading to compression of the roots of the spinal nerves. Under these conditions, osteochondrosis of the thoracic spine occurs with radical syndrome, which is a pain of various localizations (sometimes very distant) and a violation of the function of many organs of the human body (liver, lungs, pancreas, heart, etc. ).
Because of such ambiguous and varied manifestations of thoracic osteochondrosis, doctors often refer to this pathological form as "chameleon disease, " as it can cleverly disguise itself for symptoms of respiratory and gastrointestinal diseases, myocardial infarction, and so on. In this situation, a correctly performed differential diagnosis is very important to help determine the symptoms and treatment of osteochondrosis of the thoracic spine through various specialized studies.
The tactics and efficacy of further therapy are highly dependent on the extent of progression of the degenerative-dystrophic process in spinal tissues. Once the pathology is recognized in the early stages of development, significant improvement in the patient’s condition through simple physiotherapy techniques and exercise practices is entirely possible, but if detected late, complex surgery may be required. Therefore, vertebrologists recommend that you seek professional help as soon as possible for any common and / or prolonged back pain.
Pathogenesis
The incidence of osteochondrosis of the thoracic spine is virtually the same in women and men, as there is no sexual predisposition to the occurrence of intervertebral disc degeneration in the pathogenesis of this disease. Nevertheless, many years of clinical experience in the treatment of osteochondrosis indicate that the first symptoms appear earlier in men than similar negative symptoms in women. This is especially due to the fact that osteochondral tissue protects the tissues of the female body up to a certain age with the hormone estrogen, the decrease in levels of which during menopausal transformations is the cause of spinal problems.
Statistics show that intervertebral osteochondrosis is generally of varying severity in the majority of elderly people, which automatically classifies it as age-related. Meanwhile, the last time is followed by a significant "recurrence" of this pathology, until its occurrence in preschool age. For this reason, the exact etiology and initial pathogenesis of spinal osteochondrosis have not been determined to date. At one time, more than a dozen theories of its origin and development emerged, including hormonal, infectious, mechanical, vascular, hereditary, allergic, and other theories, but in practice, none of them found full confirmation.
Today, physicians explain the occurrence of osteochondrosis by the sum of complementary negative effects on spinal tissues, including constant overloads of one or more spinal movements from segments formed by an adjacent vertebra (upper and lower) and a central disc. Paradoxically, such overload is a consequence of both excessive physical work on the spine and the result of a possible long-term finding in an unnatural position for the back. For example, prolonged work or learning while sitting at a table is one of the primary factors in the development of degenerative-dystrophic changes in the structure of the intervertebral vertebra.
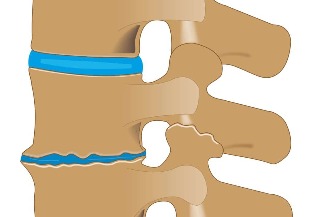
The initial development or exacerbation of osteochondrosis of the thoracic spine may be affected by malnutrition, uneven development of the back and chest muscles, overweight (obesity), pathology of the lower extremities (e. g. , flat legs), back injuries, and so on. A significant role in the pathogenesis of this disease is the disorganization of segmental circulation, which causes dehydration of the pulp (gelatinous) nucleus, which in turn results in loss of intervertebral disc damping properties, changes in surrounding fibrous ring load, and further gradual destruction of this spinal motion segment.
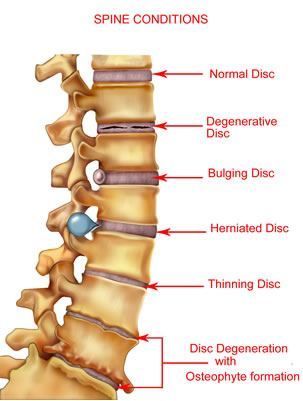
In the process of progression of thoracic osteochondrosis, it goes through 4 consecutive stages of development, each characterized by anatomical and morphological changes in the disc, adjacent vertebrae, and facial joints. In addition, negative metamorphoses with this disease can directly affect other nearby tissues (muscle, vascular system, connective tissue) or indirectly affect the work of distant organs and systems of the human body. (intestines, heart, lungs, etc. ).
First Degree
In the initial stages of the development of thoracic osteochondrosis, microcracks are formed in the inner membrane of the annulus fibrosus, into which the nucleus pulposus begins to gradually penetrate, irritating the nerve endings of the fibrous distal layers. rings and longitudinal back strip. At this stage in the development of the disease, the patient may already feel pain right in the middle of the back, or may feel apparent pain in the region of the heart. A feeling of cramping contraction may also accompany you. in the back muscles.
Second Grade
Grade 2 thoracic spinal osteochondrosis is characterized by further destruction of annular fibrosis, accompanied by instability of the spinal column resulting from excessive motility of the affected vertebrae. From the 2nd stage of the development of painful pathology, the feelings intensify and as dorsalgia (mild persistent pain aggravated by back movements) or dorsal (emerging sharply in the background of prolonged stay in one position, strong) "Shot" pains).
Third Degree
In the third period of thoracic osteochondrosis, complete rupture of the annulus fibrosus structure occurs beyond the extracellular nucleus and formation of the intervertebral hernia. Most often, such formations dive in the direction of the vertebrae, leading to compression of the spinal cord, spinal nerves, and adjacent vessels. It is accompanied by radical syndrome (radiation of pain to different parts of the body), thoracalgia underlying osteochondrosis (severe pain behind the sternum, similar heart muscle), myelopathy (sensory and motor disorders) and other neurovascular and muscle tonic symptoms. Fixed chest kyphosis, scoliosis, or kyphoscoliosis may begin at this stage.
Fourth grade
In the last stage of thoracic osteochondrosis, degenerative processes spread to the interspinous and yellow ligaments, other tissues of the spine, and nearby muscles. Intervertebral disc dystrophy progresses further, leading to scarring and further fibrosis. Deforming arthrosis develops in the lunar and intervertebral joints, osteophytes (bone growths) develop in the processes of the vertebrae. During this period of the disease, the clinical picture can be quite versatile, as the degree of damage to each disc is often different. In uncomplicated osteochondrosis, fibrosis of the problem plate may indicate a transition of the disease to a stable remission stage, but to some extent with loss of normal functionality. spine.
Causes
Chest osteochondrosis in men and women can be caused by the following predisposing factors:
- is a natural process of physiological aging accompanied by age-related changes in the structure of vertebral bone cartilage;
- genetic predisposition to abnormal formation of spinal motion segments;
- a physically inactive lifestyle that leads to back muscle dystrophy;
- strength sports that involve excessive mechanical strain on the spine (primarily weight lifting);
- spinal cord injuries (even those that have occurred in the distant past);
- endocrine disorders in the human body, disrupt the nutrition of spinal tissues;
- significantly exceeds normal body weight (obesity);
- unhealthy diet (lack of vitamins, minerals and fluids); pathology of the spine
- by unnatural bending;
- imbalance in muscle frame development;
- prolonged study or work in a sitting position with the body bent forward;
- physically difficult working conditions (inadequate lifting of weights);
- severe metabolic disorders;
- flat legs and other diseases of the lower extremities that affect the redistribution of spinal load;
- vascular diseases that damage the blood supply to the back;
- severe infectious, allergic and autoimmune processes;
- common hypothermia;
- stressful situations and nervous exhaustion;
- Bad habits and smoking.
Symptoms of Chest Spinal Osteochondrosis
Signs of thoracic osteochondrosis, due to the structural features of this segment of the spine described above, should not directly disturb the patient for a long time and should only occur if the pathological process is lateral spread and / or the back orthird degree transition. In general, all symptoms of thoracic osteochondrosis are expressed in the form of vertebral syndrome (with painful functional abnormalities of the bone cartilage of the spinal cord) and extravertebral or compression syndromes (abnormal impulses from the problematic segment of the spinal cord).
Vertebral syndromes
Vertebral symptoms of osteochondrosis of the thoracic segment of the spine are mainly manifested by two pain syndromes called dorsago and dorsalgia.
Dorsago
This is an acute and sudden onset of pain, called "lumbago, " which localizes in the interscapular space and can occur at any time. Most often, dorsago syndrome affects patients who are already in a pre-existing position with a predetermined body and a sharp change in body position. At the moment of the seizure, patients describe it as a "dagger blow" accompanied by a sharp spasm of the back muscles. In addition to severe pain, subjective feelings include back shortness of breath and significant restrictions on freedom of movement on the part of the back chest. A similar worsening of osteochondrosis with periodic seizures can take up to two weeks.
Dorsalgia
This syndrome differs from the previous one in the gradual development of uncomfortable and painful feelings that can worsen in two to three weeks. The pain associated with dorsalgia itself is not so pronounced, but its prolonged presence is caused by a constant feeling of anxiety. The back muscles as well as the back muscles are exposed to significant stress, which can make the patient feel a lack of inhaled air. Back pain increases with torso movement (especially when bending), deep breathing, coughing, etc. Separately, upper dorsalgia (the main localization of negative phenomena in the cervicothoracic segment of the spine) and lower dorsalgia (the main localization of negative phenomena in the thoracolumbar segment of the spine).
Extravertebral syndromes
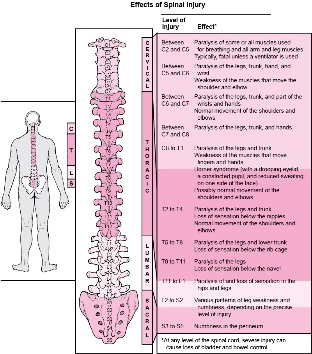
The extravertebral syndromes of thoracic osteochondrosis can be very diverse due to the largest extent of this part of the spine, which makes it very difficult to correctly diagnose the disease. As a mechanical result, appropriate nerve roots, nearby blood vessels, or the spinal cord itself would be compressed. Compression symptoms are generally similar in men and women and differ only if the abnormal impulses are spherical in nature (e. g. , erectile dysfunction is sometimes seen in the background of the disease in men). In almost all cases, extravertebral symptoms are caused by hernias between already formed vertebrae, which are most often the lower thoracic regions, but can in principle develop in any spinal motion segment from the D1 vertebra to the D12 vertebra. As shown in the image below, it is the localization of the osteochondrosis within them is the process of certain systems and organs of the pathological human body with their negative manifestations.
Radical Syndromes
Within the framework of the compression symptoms of thoracic osteochondrosis, radical syndromes are most commonly and clearly observed, caused by compression of nerve endings in one or another segment of the spine. Depending on the concentration, the problems of such patients may be disturbed by the following painful phenomena:
- In case of violation of the area of the T1 vertebra - painful sensations and paraesthesias from the movement segment of the upper thoracic spine most often extend along the suprascapular zone to the area of one armpit to the elbow joint;
- in the case of violation of the area of the T2-T6 vertebrae - pain similar to intervertebral neuralgia may extend from this part of the spine along the interscapular region and surround the axillary and scapular zones in a semicircle and 2-6 intercostal areas of the sternum;
- in case of violation of the vertebral area of T7-T8 - the belt pain spreads mainly from the lower level of the shoulder blades to the upper parts of the rib arch and affects the epigastric region where it causes muscle protection (strong muscle tension);
- in the T9-T10 vertebral region of the lesion - intercostal neuralgia extends from the lower thoracic spine movement segments to the lower ribs and the umbilical region, altering the tone of the mid-abdominal muscles;
- Injury to the T11-T12 vertebral region - pain also results from the movement segment of the lower chest spine and reaches the hypogastric (below the stomach) and lumbar regions along the corresponding lateral zones of the chest.
In addition to pain, radical syndromes of thoracic osteochondrosis often present with negative symptoms of certain internal organs of the abdomen and / or chest. Moreover, in some cases, such symptoms are so similar to the pathological manifestations of other diseases that it is virtually impossible to accurately recognize their debt without directed research. For example, the medical literature describes unreasonable behavior in gastrointestinal surgery (surgery to remove the appendix) according to a clear clinic of acute appendicitis, which has actually proven to be a pronounced syndrome of osteochondrosis.
Thus, when the process of osteochondrosis is localized in the upper thoracic region of the spine (T1 to T4), patients may experience pain and / or various discomforts in the esophagus or pharynx, often in the presence of a foreign body. Such feelings are often paroxysmal (sometimes permanent) and worsen, placing a heavy strain on the problematic part of the back. Occasionally, manifestations of radical syndrome of the upper chest segment are confused with signs of obstructive bronchitis or pneumonia, as reflex cough and chest pain associated with osteochondrosis of the thoracic region are similar to the symptoms of this disease group. In addition, chest pain may present in the form of thoracalgia, the intensity of which is reminiscent of angina pectoris, pulmonary thromboembolism, myocardial infarction attack, and other similar pathologies of a severe nature that require detailed differential analysis from physicians.
Patients with osteochondrosis of the middle part of the thoracic spine (T5 - T7) most often experience discomfort and pain in the solar plexus and stomach, called vertebrogenic gastralgia. The defeated naval movement segments, T8-T9, are possible pain in the duodenal region, called spinal duodenalgia. . . Both these and other painful feelings in different patients or at different times of intensity can vary from mild to "painful" and extremely acute. They usually increase when the body is in a position for a longer period of time (sitting at a table, lying on its back, etc. ), in case of sudden exercise, and also at the moment of sneezing or coughing. These pains are often accompanied by paraesthesia. (numbness, tingling, burning) in the middle of the abdominal wall.
Radical manifestations of osteochondrosis in the lower thoracic region of the spine (T8 to T12) Some patients may complain of lower abdominal pain, mimicking intestinal disorders or pathology. Sometimes the pain spreads to the gallbladder and is localized in the posterior region of the right hypochondrium. Even less rarely, patients in the suprapubic region experience pain similar to that of an abnormal bladder clinic. As before, the nature of such pain can vary over a fairly wide range (between mild and intense) and their severity can be accompanied by prolonged physical or static stress on the spine, sneezing, coughing, and so on.
Compression myelopathy
This compression syndrome in thoracic osteochondrosis is quite rare and results directly from spinal cord compression resulting in intervertebral hernia. . . Typical symptoms of early onset of development include local pain in the appropriate area of the back or belt in the problem area, as well as a feeling of weakness and / or numbness in the legs. With progression, the pain increases, can affect the intervertebral space, abdominal organs, lumbar area and is significantly felt in the lower extremities. In severe cases with compression myelopathy, pelvic organ dysfunction may occur, which may lead to disruption of defecation and / or urination. In addition, there may be severe superficial and deep paraesthesias and sensory disturbances, all the way to spastic paresis in one or even both legs.
Vascular compression
Compression of blood vessels adjacent to the thoracic segment of the spine leads to myeloischemia, which results in disruption of the blood supply and thus proper nutrition of the spinal cord. Manifestations of this syndrome are indeed a complete recurrence of compression myelopathy symptoms characterized mainly by pelvic disorders as well as loss of lower limb sensation and loss of function. Patients often describe the problem with the term "legs fail. "
Vegetative syndromes
In many cases, chest osteochondrosis causes damage to the vegetative nerve nodes (ganglia), which can cause the patient to experience a variety of negative symptoms. These can be different paresthesias. , itching and changes in skin pigmentation in the problematic ganglion, burning pain in one half of the body, local temperature abnormalities, excessive or exhausted muscle, disorder in the work of limbs or internal organs, etc. In his view, these visceral vertebrogenic symptoms are similar to the manifestations of radical syndromes, but differ from them in the absence of clear localization and in the presence of secretory and locomotor disorders. When a node involving the upper thoracic vertebrae is involved in the pathological process of a star star, there may be injuries to the arms, upper chest, and heart. Injury to the lower thoracic ganglia can result in functional disorders of the pelvis, abdominal and thoracic organs, and trophic changes in the lower extremities and the rest of the body.